
D2 Radical Distal Gastrectomy for Gastric Cancer.
A D2 lymphadenectomy is the standard radical nodal dissection performed during curative gastrectomy for many resectable gastric cancers, especially in East Asian surgical practice and increasingly worldwide in experienced centers.
It means removal of:
- Perigastric lymph nodes (D1 stations)
PLUS
- Second-tier nodes along major arteries supplying the stomach
The goal is:
- Better oncologic clearance
- More accurate staging
- Improved locoregional control
- Potential survival benefit in appropriately selected patients
⸻
1. Definition
D1 Dissection
Removes only perigastric nodes immediately adjacent to the stomach.
D2 Dissection
Removes D1 nodes PLUS nodes along:
- Left gastric artery
- Common hepatic artery
- Celiac axis
- Splenic artery
- Hilum of spleen (in selected total gastrectomy cases)
⸻
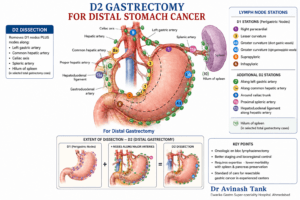
2. Lymph Node Stations (Japanese Classification)
D1 Stations
Distal Gastrectomy
- Station 1: Right paracardial
- Station 3: Lesser curvature
- Station 4sb/4d: Greater curvature
- Station 5: Suprapyloric
- Station 6: Infrapyloric
⸻
Additional D2 Stations
For distal gastrectomy:
- Station 7 → Along left gastric artery
- Station 8a → Along common hepatic artery
- Station 9 → Around celiac trunk
- Station 11p → Proximal splenic artery
- Station 12a → Hepatoduodenal ligament along hepatic artery
This is why the left gastric artery is usually divided at its origin during D2 dissection:
- To completely clear station 7 nodes.
⸻
3. Indications for D2 Lymphadenectomy
Generally recommended for:
- Resectable gastric adenocarcinoma
- ≥T2 lesions
- Node-positive disease
- Many T1 cancers with high-risk features
Usually performed when:
- Patient is fit
- Surgery done in experienced high-volume centers
⸻
4. Extent According to Surgery Type
Distal Gastrectomy
D2 includes:
1, 3, 4sb, 4d, 5, 6, 7, 8a, 9, 11p, 12a
Total Gastrectomy
Adds:
- 2
- 4sa
- 10 (sometimes selective)
- 11d
⸻
5. Historical Controversy
Older Western trials showed:
- Higher morbidity
- Higher mortality
Mainly because:
- Routine splenectomy
- Routine distal pancreatectomy
Modern modified D2 surgery:
- Preserves pancreas and spleen unless directly involved
- Has much lower complications
- Now accepted standard in expert centers
⸻
6. Current Standard Practice
In East Asia
D2 = standard of care.
In Europe
Widely accepted in specialized units.
In North America
Recommended in experienced centers.
Guidelines from:
- Japanese Gastric Cancer Association
- NCCN
- ESMO
support D2 dissection for appropriate resectable cancers.
⸻
7. Technical Principles
Key operative components:
- En bloc nodal clearance
- High ligation of vessels
- Sharp dissection along vascular planes
- Omentectomy (depending on stage)
- Adequate proximal/distal margins
⸻
8. Important Vascular Steps
During distal gastrectomy:
- Right gastroepiploic vessels divided
- Right gastric artery divided
- Usually left gastric artery ligated at root
- Left gastroepiploic may or may not be preserved depending on extent
⸻
9. Morbidity Risks
Potential complications:
- Pancreatic fistula
- Bleeding
- Anastomotic leak
- Delayed gastric emptying
- Splenic injury
Risk strongly depends on:
- Surgical expertise
- Hospital volume
⸻
10. Adequate Nodal Yield
Recommended:
- At least 16 nodes for staging
- D2 commonly yields 25–40+ nodes
Higher nodal yield improves:
- Accurate TNM staging
- Adjuvant treatment planning
⸻
11. Minimally Invasive D2 Gastrectomy
Increasingly performed via:
- Laparoscopic gastrectomy
- Robotic gastrectomy
Benefits may include:
- Less blood loss
- Faster recovery
- Similar oncologic outcomes in experienced hands
⸻
12. Key Modern Concept
Modern gastric cancer surgery is shifting toward:
- Precision lymphadenectomy
- Function preservation in early cancers
- Sentinel node concepts
- Fluorescence-guided surgery (ICG)
But for standard resectable advanced antral cancer:
Distal gastrectomy with D2 lymphadenectomy remains the benchmark oncologic operation.
………
Surgical Principles, Techniques & Reconstruction of D2 Radical Distal Gastrectomy for Gastric Cancer
Introduction
Gastric cancer remains one of the leading causes of cancer-related mortality worldwide. Surgery continues to be the cornerstone of curative treatment for localized stomach cancer. Among various operative procedures, D2 Radical Distal Gastrectomy is considered the gold-standard surgery for cancers involving the distal third (antrum and pylorus) of the stomach in appropriately selected patients.
The operation combines:
- Adequate oncologic gastric resection
- Systematic lymph node dissection
- Safe reconstruction of gastrointestinal continuity
The success of this surgery depends not only on removing the tumor but also on respecting precise anatomical planes, achieving oncological clearance, preserving physiological function whenever possible, and minimizing postoperative complications.
Understanding Distal Gastric Cancer
Distal gastric cancers arise in:
- Gastric antrum
- Pylorus
- Lower body of stomach
These tumors commonly spread through:
- Submucosal lymphatic channels
- Regional perigastric nodes
- Nodes along major abdominal vessels
Therefore, treatment requires:
- Removal of the tumor-bearing stomach segment
- Adequate proximal and distal margins
- Radical lymphadenectomy
This forms the basis of D2 radical surgery.
What is D2 Radical Distal Gastrectomy?
A Distal Gastrectomy removes:
- Distal part of stomach
- Antrum
- Pylorus
- Variable portion of gastric body
A D2 lymphadenectomy means:
- Removal of D1 perigastric nodes
PLUS - Removal of second-tier lymph nodes along major arteries supplying the stomach.
Surgical Principles of D2 Radical Gastrectomy
1. Oncologic En Bloc Resection
The tumor and lymphatic drainage basin should be removed together as one specimen without tumor violation.
Principles include:
- No tumor handling
- Clear circumferential planes
- Adequate resection margins
- Sharp anatomical dissection
2. Adequate Resection Margin
Recommended margins generally include:
- 3–5 cm for intestinal-type tumors
- Larger margins for diffuse-type tumors
Frozen section may be used when margins are doubtful.
3. Systematic Lymphadenectomy
The hallmark of D2 surgery is systematic nodal dissection.
D1 Stations
- 1
- 3
- 4sb
- 4d
- 5
- 6
Additional D2 Stations
- 7: Left gastric artery
- 8a: Common hepatic artery
- 9: Celiac trunk
- 11p: Proximal splenic artery
- 12a: Hepatoduodenal ligament
The goal is:
- Better staging
- Improved local control
- Potential survival benefit
4. Preservation of Non-involved Organs
Modern D2 surgery avoids unnecessary:
- Splenectomy
- Distal pancreatectomy
unless directly invaded by tumor.
This has significantly reduced:
- Morbidity
- Pancreatic fistula
- Mortality
5. Respect for Embryological Planes
Dissection follows avascular fascial planes:
- Suprapancreatic plane
- Mesogastric fascial layers
- Vascular sheaths
This improves:
- Safety
- Completeness of nodal clearance
- Reduced bleeding
Operative Techniques of D2 Radical Distal Gastrectomy
Preoperative Preparation
Clinical Assessment
Includes:
- Nutritional evaluation
- Comorbidity optimization
- Anesthetic fitness
Investigations
- Upper GI endoscopy with biopsy
- Contrast-enhanced CT scan
- PET-CT in selected cases
- Diagnostic laparoscopy in advanced disease
Patient Positioning
Usually:
- Supine position
- Legs apart (French position in laparoscopy)
- Reverse Trendelenburg
Surgical Approaches
1. Open Gastrectomy
Traditional approach.
Advantages:
- Tactile feedback
- Easier in bulky tumors
2. Laparoscopic Gastrectomy
Increasingly accepted.
Advantages:
- Less pain
- Early recovery
- Reduced blood loss
Requires advanced expertise.
3. Robotic Gastrectomy
Offers:
- Better dexterity
- Precision dissection
- Superior ergonomics
Especially useful in:
- Suprapancreatic lymphadenectomy
Step-by-Step Operative Technique
Step 1: Exploration
Abdominal cavity examined for:
- Liver metastasis
- Peritoneal deposits
- Ascites
- Omental disease
Peritoneal cytology may be taken.
Step 2: Omentectomy
Greater omentum divided:
- Usually 3–5 cm away from gastroepiploic arcade
- Transverse colon protected
Step 3: Infrapyloric Node Dissection (Station 6)
Right gastroepiploic vessels identified and divided at origin.
Careful preservation of:
- Pancreatic head
- Colic vessels
Step 4: Suprapyloric Dissection (Station 5)
Right gastric artery ligated.
Nodes over:
- Proper hepatic artery
- Suprapyloric region removed
Step 5: Duodenal Transection
First part of duodenum divided using:
- Linear stapler
or - Hand-sewn technique
Adequate distal margin ensured.
Step 6: Lesser Curvature Dissection
Nodes along lesser curvature cleared.
Includes:
- Station 3 nodes
Step 7: Left Gastric Artery Dissection (Station 7)
One of the most important steps.
The:
- Left gastric vein divided
- Left gastric artery ligated at origin
This permits:
- Complete station 7 dissection
Step 8: Common Hepatic Artery Nodes (8a)
Lymphatic tissue cleared along:
- Common hepatic artery
Step 9: Celiac Axis Nodes (9)
Soft tissue around celiac trunk dissected meticulously.
Step 10: Splenic Artery Nodes (11p)
Dissection along proximal splenic artery.
Care taken to avoid:
- Pancreatic injury
- Splenic vessel trauma
Step 11: Gastric Transection
Stomach divided proximally ensuring adequate margin.
Reconstruction After Distal Gastrectomy
Reconstruction restores GI continuity after resection.
Choice depends on:
- Tumor location
- Residual stomach
- Patient condition
- Surgeon preference
1. Billroth I Reconstruction (Gastroduodenostomy)
Technique
Remnant stomach directly anastomosed to duodenum.
Advantages
- Physiological pathway preserved
- Less nutritional disturbance
Limitations
- Requires tension-free anastomosis
- Difficult after extensive resection
Complications
- Bile reflux
- Anastomotic tension
2. Billroth II Reconstruction (Gastrojejunostomy)
Technique
Stomach connected to proximal jejunum.
Advantages
- Technically easier
- Useful when duodenum not mobile
Disadvantages
- Bile reflux gastritis
- Afferent loop syndrome
- Dumping syndrome
3. Roux-en-Y Reconstruction
Currently preferred in many centers.
Technique
- Gastrojejunostomy created
- Roux limb fashioned
- Jejunojejunostomy added
Advantages
- Less bile reflux
- Better quality of life
- Reduced gastritis
Disadvantages
- Technically complex
- Roux stasis syndrome possible
Stapled vs Hand-Sewn Anastomosis
Both techniques are acceptable.
Stapled Anastomosis
Advantages:
- Faster
- Consistent lumen
- Less operative time
Hand-Sewn Anastomosis
Advantages:
- Better customization
- Useful in difficult anatomy
Enhanced Recovery After Surgery (ERAS)
Modern perioperative care includes:
- Early mobilization
- Early feeding
- Multimodal analgesia
- DVT prophylaxis
- Minimal drains/tubes
Benefits:
- Shorter hospital stay
- Faster recovery
- Reduced complications
Complications of D2 Distal Gastrectomy
Early Complications
- Bleeding
- Anastomotic leak
- Pancreatic fistula
- Intra-abdominal abscess
Late Complications
- Dumping syndrome
- Nutritional deficiency
- Iron deficiency anemia
- Vitamin B12 deficiency
- Bile reflux
Nutritional Considerations
Patients require:
- Small frequent meals
- High-protein diet
- Vitamin supplementation
- Long-term follow-up
Nutritional rehabilitation is critical after gastrectomy.
Oncologic Outcomes
When performed properly in experienced centers, D2 gastrectomy provides:
- Better nodal staging
- Improved locoregional control
- Potential survival benefit
Adequate lymph node retrieval:
- Usually >25 nodes
Future Advances in Gastric Cancer Surgery
Modern innovations include:
- ICG fluorescence-guided lymphatic mapping
- Sentinel node navigation surgery
- Function-preserving gastrectomy
- Robotic suprapancreatic dissection
- Precision surgery based on molecular biology
Conclusion
D2 Radical Distal Gastrectomy represents a sophisticated balance between:
- Radical oncologic clearance
- Anatomical precision
- Functional preservation
The operation demands:
- Detailed anatomical understanding
- Advanced surgical expertise
- Careful perioperative management
With modern refinements, pancreas-preserving and spleen-preserving D2 gastrectomy has become a safe and effective standard treatment for distal gastric cancer in specialized centers.
Proper reconstruction and postoperative rehabilitation are equally important for ensuring:
- Good nutritional recovery
- Better quality of life
- Long-term oncologic success
About the Author
Dr. Avinash Tank
MS, MCh (SGPGIMS)
Consultant GI, HPB & Bariatric Surgeon
Dwarika Gastro Super-speciality Hospital

Super-specialist GI, bariatric & cancer surgeon. SGPGIMS (India's premier GI centre) + advanced training in Japan & South Korea. Read full profile →
Last reviewed: July 2026



Comments
Be the first to share your thoughts on this article.