Reading Time: 8 minutes
Why Traditional Diabetes Tests May Miss Early Disease Understanding the New Era of Diabetes Detection
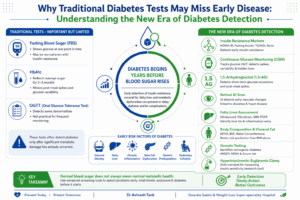
For decades, diabetes diagnosis has relied primarily on three laboratory tests: fasting blood glucose, postprandial blood glucose, and glycated hemoglobin (HbA1c).
These tests have undoubtedly transformed diabetes care and helped millions of patients receive timely treatment.
However, emerging scientific evidence suggests that diabetes begins many years before blood sugar levels become abnormal.
By the time fasting glucose or HbA1c rises above diagnostic thresholds, significant metabolic damage may have already occurred.
Researchers now recognize that insulin resistance, visceral obesity, fatty liver disease, chronic inflammation, and genetic predisposition often develop years before overt hyperglycemia appears.
This evolving understanding has led to the development of newer diagnostic tools that can identify metabolic dysfunction earlier than traditional glucose measurements.
The future of diabetes diagnosis is moving beyond simply measuring blood sugar and toward evaluating overall metabolic health.
Why Traditional Diabetes Tests Have Limitations
Fasting Blood Sugar (FBS)
Fasting blood sugar measures glucose levels after at least 8 hours of fasting.
Advantages
- Easy to perform
- Widely available
- Inexpensive
- Useful for diagnosing established diabetes
Limitations
Many individuals maintain normal fasting glucose despite significant insulin resistance.
The pancreas initially compensates for insulin resistance by producing more insulin. During this compensation phase, fasting glucose may remain normal for years while metabolic damage continues silently.
Thus, a normal fasting sugar report does not always indicate optimal metabolic health.
HbA1c: The Three-Month Sugar Report Card
HbA1c reflects average blood glucose levels during the previous 2–3 months.
An HbA1c level:
- Below 5.7% = Normal
- 5.7–6.4% = Prediabetes
- ≥6.5% = Diabetes
Why HbA1c Can Miss Early Diabetes
HbA1c measures average glucose but fails to reveal:
- Post-meal glucose spikes
- Daily glucose fluctuations
- Nocturnal hypoglycemia
- Early insulin resistance
A patient may experience repeated post-meal glucose surges while maintaining a normal HbA1c level.
Studies suggest that postprandial hyperglycemia contributes significantly to vascular damage and cardiovascular risk.
Diabetes Begins with Insulin Resistance
What Is Insulin Resistance?
Insulin acts like a key that allows glucose to enter cells.
In insulin resistance:
- Cells become less responsive to insulin.
- The pancreas compensates by producing more insulin.
- Blood sugar remains normal initially.
- Over time, pancreatic beta cells become exhausted.
- Diabetes eventually develops.
The problem is that traditional diabetes tests often identify disease only after this compensation mechanism begins to fail.
HOMA-IR: Detecting Insulin Resistance Before Diabetes
What Is HOMA-IR?
HOMA-IR stands for Homeostatic Model Assessment of Insulin Resistance.
It is calculated using:
- Fasting glucose
- Fasting insulin
Formula
HOMA-IR = Fasting Insulin × Fasting Glucose ÷ 405
What Does It Tell Us?
Higher values indicate greater insulin resistance.
Clinical Importance
Research demonstrates that elevated HOMA-IR predicts:
- Future diabetes
- Fatty liver disease
- Cardiovascular disease
- Metabolic syndrome
Many individuals show elevated HOMA-IR years before diabetes develops.
Advantages
- Simple blood test
- Inexpensive
- Early identification of high-risk individuals
Limitations
- No universal cutoff value
- Results may vary among populations
Triglyceride-to-HDL Ratio: A Simple Yet Powerful Marker
Why This Ratio Matters
Insulin resistance affects fat metabolism long before glucose levels become abnormal.
Typical findings include:
- Elevated triglycerides
- Reduced HDL cholesterol
The triglyceride-to-HDL ratio therefore acts as a surrogate marker of insulin resistance.
Clinical Significance
Several studies have shown that a high TG/HDL ratio correlates with:
- Metabolic syndrome
- Type 2 diabetes
- Cardiovascular disease
- Visceral obesity
Benefits
- Easily calculated
- No additional testing cost
- Available from routine lipid profiles
The Hidden Danger of Visceral Fat
Not All Fat Is Equal
Most people focus on body weight.
However, the location of fat may be more important than the total amount.
Subcutaneous Fat
Located under the skin.
Visceral Fat
Located around internal organs.
Visceral fat is metabolically active and produces inflammatory chemicals called adipokines.
These include:
- TNF-alpha
- IL-6
- Resistin
These substances promote:
- Insulin resistance
- Chronic inflammation
- Endothelial dysfunction
- Cardiovascular disease
Body Composition Analysis: Looking Beyond BMI
The Problem with BMI
Body Mass Index (BMI) does not distinguish:
- Muscle from fat
- Visceral fat from subcutaneous fat
A person may have:
- Normal BMI
- Excess visceral fat
- Significant metabolic risk
This phenomenon is known as “TOFI” (Thin Outside, Fat Inside).
Modern Body Composition Assessment
Techniques include:
Bioelectrical Impedance Analysis (BIA)
Measures:
- Body fat percentage
- Muscle mass
- Visceral fat estimation
DEXA Scan
Dual-energy X-ray absorptiometry provides highly accurate measurement of:
- Fat mass
- Lean mass
- Bone density
- Visceral adiposity
Many researchers now consider DEXA superior to BMI for metabolic risk assessment.
Fatty Liver: The Earliest Sign of Metabolic Disease
What Is Non-Alcoholic Fatty Liver Disease (NAFLD)?
NAFLD occurs when fat accumulates inside liver cells.
Today, experts increasingly use the term:
Metabolic Dysfunction-Associated Steatotic Liver Disease (MASLD).
Why It Matters
Studies suggest fatty liver often appears before diabetes develops.
The liver becomes resistant to insulin and begins releasing excessive glucose into the bloodstream.
This contributes to:
- Prediabetes
- Type 2 diabetes
- Cardiovascular disease
Diagnostic Tests
Ultrasound
Most commonly used.
FibroScan
Measures:
- Liver stiffness
- Liver fat content
MRI-PDFF
Most accurate imaging technique for liver fat quantification.
Presence of fatty liver significantly increases future diabetes risk.
Newer Options
Continuous Glucose Monitoring (CGM): Seeing What HbA1c Cannot
What Is Continuous Glucose Monitoring?
Continuous Glucose Monitoring (CGM) is a revolutionary technology that measures glucose levels continuously throughout the day and night using a small sensor placed under the skin.
Unlike traditional blood sugar testing, which provides only a single snapshot, CGM records glucose readings every few minutes, generating hundreds of measurements daily.
This allows physicians to observe real-world glucose patterns and fluctuations that conventional tests often miss.
How Does CGM Work?
A tiny sensor inserted beneath the skin measures glucose levels in the interstitial fluid.
The sensor transmits readings to:
- Smartphone applications
- Dedicated receivers
- Insulin pumps
Many modern CGM systems provide readings every 1–5 minutes.
Popular systems include:
- FreeStyle Libre
- Dexcom G7
- Medtronic Guardian
What Important Information Does CGM Reveal?
1. Post-Meal Glucose Spikes
Many individuals maintain normal fasting glucose but experience substantial glucose surges after meals.
These spikes contribute to:
- Oxidative stress
- Inflammation
- Endothelial dysfunction
- Cardiovascular disease
CGM can identify these hidden abnormalities.
2. Glycemic Variability
Blood sugar fluctuations themselves may contribute to diabetic complications independent of average glucose levels.
Research suggests excessive glycemic variability increases:
- Oxidative stress
- Vascular injury
- Risk of complications
HbA1c cannot measure glucose variability.
CGM can.
3. Nocturnal Hypoglycemia
Many patients experience low glucose levels during sleep without realizing it.
CGM alerts patients and physicians to:
- Overnight glucose drops
- Dawn phenomenon
- Early morning hyperglycemia
4. Time in Range (TIR)
Modern diabetes management increasingly emphasizes Time in Range.
This refers to the percentage of time glucose remains within target values.
A higher Time in Range is associated with fewer diabetic complications.
1,5-Anhydroglucitol (1,5-AG): Detecting Hidden Glucose Excursions
What Is 1,5-Anhydroglucitol?
1,5-Anhydroglucitol (1,5-AG) is a naturally occurring sugar-like molecule found in food and blood.
Its concentration decreases when glucose levels rise significantly.
Why Is It Useful?
HbA1c reflects average glucose over approximately three months.
However, HbA1c may remain normal despite repeated post-meal glucose spikes.
1,5-AG is particularly sensitive to:
- Short-term hyperglycemia
- Postprandial glucose excursions
- Early glucose abnormalities
Clinical Applications
Useful in:
- Prediabetes
- Early Type 2 diabetes
- Monitoring dietary interventions
- Evaluating unexplained glucose fluctuations
Several studies have demonstrated that low 1,5-AG levels correlate with increased cardiovascular risk and glycemic variability.
Retinal AI Scans: Can the Eye Reveal Diabetes?
The Retina as a Window to Metabolic Health
The retina contains a dense network of tiny blood vessels.
Diabetes often affects these vessels long before symptoms appear.
Traditionally, retinal examinations have been used to detect diabetic retinopathy.
Artificial Intelligence is now expanding the potential of retinal imaging.
How Does AI-Based Retinal Screening Work?
Advanced algorithms analyze retinal photographs and identify subtle patterns invisible to the human eye.
AI systems can estimate:
- Diabetes risk
- Cardiovascular risk
- Biological age
- Blood pressure trends
Researchers believe retinal imaging may eventually become a rapid non-invasive metabolic screening tool.
Advantages
- Completely non-invasive
- Quick procedure
- No blood sample required
- Potential for mass screening
Iris Analysis and Emerging Technologies
Researchers are investigating whether changes in the iris and ocular microcirculation may provide additional metabolic information.
Although still under development, these technologies could someday assist in:
- Diabetes screening
- Cardiovascular risk assessment
- Early disease prediction
Currently, retinal imaging has significantly stronger scientific evidence than iris-based approaches.
Hyperinsulinemic-Euglycemic Clamp: The Gold Standard
What Is It?
The Hyperinsulinemic-Euglycemic Clamp Technique is considered the most accurate method available for measuring insulin sensitivity.
Because of its complexity, it is primarily used in research settings.
How Is It Performed?
Two intravenous infusions are administered:
Insulin Infusion
Raises insulin levels to a controlled high concentration.
Glucose Infusion
Maintains normal blood glucose levels.
The amount of glucose required reflects how sensitive the body is to insulin.
Why Is It Important?
This technique directly measures insulin action.
It provides:
- Precise assessment of insulin sensitivity
- Accurate measurement of insulin resistance
- Validation for other diagnostic tests
Most newer insulin resistance markers are compared against clamp studies.
Genetic Testing: The Future of Precision Diabetes Medicine
Not All Diabetes Is the Same
Traditional classification includes:
- Type 1 Diabetes
- Type 2 Diabetes
- Gestational Diabetes
Modern genetic research has revealed multiple additional forms of diabetes.
Neonatal Diabetes Mellitus (NDM)
Neonatal Diabetes Mellitus is a rare condition occurring during the first months of life.
Unlike classic Type 1 diabetes, NDM often results from specific genetic mutations.
Why Genetic Testing Matters
A precise genetic diagnosis may:
- Identify the exact cause
- Predict disease progression
- Guide treatment decisions
- Prevent unnecessary lifelong insulin therapy
Some genetic forms respond dramatically to oral medications instead of insulin.
MODY: Maturity-Onset Diabetes of the Young
What Is MODY?
MODY is a hereditary form of diabetes caused by mutations in specific genes affecting insulin secretion.
It is frequently misdiagnosed as Type 1 or Type 2 diabetes.
Common MODY Genes
- HNF1A
- HNF4A
- GCK
- HNF1B
Accurate diagnosis can dramatically alter treatment strategies.
The Emerging Concept of Diabetes Subtypes
Scientists increasingly believe diabetes represents a spectrum rather than a single disease.
Type 3 Diabetes
The term Type 3 Diabetes is often used to describe the relationship between insulin resistance and Alzheimer’s disease.
Research suggests impaired brain insulin signaling may contribute to cognitive decline.
This remains an area of active investigation.
Type 4 Diabetes
Some researchers have proposed Type 4 Diabetes as a form occurring in lean older adults with age-related insulin resistance.
The concept remains under study.
Type 5 Diabetes
Recently recognized by international diabetes experts, Type 5 Diabetes has been linked to malnutrition-associated diabetes.
It is most commonly seen in low-income regions where childhood malnutrition remains prevalent.
These patients often have:
- Low body weight
- Reduced insulin production
- Distinct metabolic characteristics
Recognition of Type 5 Diabetes highlights the complexity of diabetes beyond obesity alone.
Why Visceral Fat Is More Dangerous Than High Blood Sugar
The Inflammatory Organ You Never Knew You Had
Visceral fat is now considered an endocrine organ.
It secretes numerous inflammatory substances including:
- Tumor Necrosis Factor-alpha (TNF-α)
- Interleukin-6 (IL-6)
- Monocyte Chemoattractant Protein-1 (MCP-1)
These molecules contribute to:
- Insulin resistance
- Fatty liver
- Hypertension
- Atherosclerosis
- Type 2 diabetes
Many experts now believe visceral fat measurement should become a routine component of metabolic assessment.
A New Comprehensive Diabetes Risk Assessment Model
The future of diabetes screening may combine:
Traditional Tests
- Fasting glucose
- HbA1c
- Oral glucose tolerance test
Advanced Metabolic Markers
- HOMA-IR
- Fasting insulin
- TG/HDL ratio
- 1,5-AG
Body Composition Assessment
- DEXA
- BIA
- Waist circumference
- Visceral fat measurement
Liver Health Assessment
- Ultrasound
- FibroScan
- Liver enzymes
Advanced Monitoring
- Continuous Glucose Monitoring
Precision Medicine
- Genetic testing
- AI-based retinal analysis
Together, these tools can identify metabolic dysfunction years before conventional diabetes develops.
Practical Clinical Message
The greatest misconception in diabetes care is the belief that normal blood sugar automatically means normal metabolic health.
A patient may have:
- Insulin resistance
- Fatty liver
- Visceral obesity
- Elevated fasting insulin
- Chronic inflammation
while maintaining normal glucose values.
By the time blood sugar becomes abnormal, significant metabolic damage may already have occurred.
The future of diabetes prevention lies in identifying metabolic dysfunction early and intervening before irreversible complications develop.
Conclusion
Diabetes diagnosis is undergoing a paradigm shift. Modern medicine is moving beyond a simple glucose-centered model toward a comprehensive assessment of metabolic health.
Continuous glucose monitoring, HOMA-IR, triglyceride-to-HDL ratio, body composition analysis, fatty liver assessment, retinal AI screening, and genetic testing are expanding our ability to detect disease earlier than ever before.
For clinicians and patients alike, the message is clear:
Don’t wait for diabetes to appear. Detect metabolic dysfunction early, treat insulin resistance aggressively, reduce visceral fat, improve liver health, and prevent diabetes before it begins.
The future of diabetes care is not merely controlling blood sugar—it is preserving metabolic health.
Why Traditional Diabetes Tests May Miss Early Disease: Understanding the New Era of Diabetes Detection
Dr. Avinash Tank
Dwarika Gastro & Weight Loss Super-speciality Hospital
Authentic PubMed References
- Matthews DR, Hosker JP, Rudenski AS, et al. Homeostasis model assessment (HOMA). Diabetologia. 1985. PMID: 3899825
- DeFronzo RA. From the Triumvirate to the Ominous Octet. Diabetes. 2009. PMID: 19336687
- Monnier L, Colette C. Glycemic variability. Diabetes Care. 2008. PMID: 18227457
- Bergenstal RM et al. Clinical targets for continuous glucose monitoring. Diabetes Care. 2018. PMID: 29678883
- Cusi K. Treatment of NAFLD in Type 2 Diabetes. Diabetologia. 2016. PMID: 27220603
- Neeland IJ et al. Visceral adiposity and cardiometabolic risk. Circulation. 2019. PMID: 30586753
- Yamanouchi T et al. Clinical usefulness of 1,5-Anhydroglucitol. Diabetes Care. 1991. PMID: 1884618
- American Diabetes Association. Standards of Care in Diabetes. Updated annually.
- Hattersley AT, Patel KA. Precision diabetes and monogenic diabetes. Lancet. 2017. PMID: 28190536
- Tuomi T, Santoro N, Caprio S, et al. The many faces of diabetes. Lancet. 2014. PMID: 24315621
- Gastaldelli A. Fatty liver and insulin resistance. Current Diabetes Reports. 2022. PMID: 35091888
- Kahn SE, Hull RL, Utzschneider KM. Mechanisms linking obesity to insulin resistance and Type 2 diabetes. Nature. 2006. PMID: 17167471.